Why Radiographic Findings Must Match the Horse: When “Normal” Isn’t Enough
This interpretation framework reflects referral-level radiological assessment used in equine lameness practice, including case review, second-opinion reporting, and longitudinal follow-up of sport horses.
Reviewed against current reference standards and updated to reflect contemporary equine diagnostic imaging for veterinarians practice.
The horse is lame and lameness is abolished by palmar digital nerve blocks. You’ve acquired what you think is a good set of radiographs but you are unable to detect any radiological abnormality.
You went back and blocked the navicular bursa and the lameness improved.
So what now?
Or maybe it’s the opposite. There are many radiographic abnormalities – multiple large and variably shaped synovial invaginations; some increase in opacity of the spongiosa; questionable irregularity of the palmar margin of the palmar compact bone.
But the horse is sound and competing, without any history of medication and without any special pads or shoes.
This is where real diagnostic confidence begins – not with the radiograph, but with the ability to interpret it in context – and the realisation that we do not necessarily understand what causes pain and lameness.
Moreover there is not a single definition of navicular disease, nor can the navicular bone be considered in isolation.
Radiographs are not definitive. They’re a tool. And like any tool, their value depends on their quality and how they’re used.
In this final article before the live masterclass with Dr. Sue Dyson, we’re not introducing another radiographic feature. You’ve already learned the key ones – changes in shape of the bone, the significance or otherwise of synovial invaginations, palmar compact bone irregularities, increased opacity of the spongiosa.
Now it’s time to bring them together and ask the bigger question:
Does what I see on the screen match the horse in front of me? That’s the question every good lameness equine veterinarian learns to ask. Because when it doesn’t – the radiograph isn’t wrong. It’s just not the whole story.

Radiographs Are a Tool – Not the Answer
Radiographs are central to the diagnostic workup of palmar foot pain. But they are not definitive. They reveal structure, not pain.
And in many cases, structure doesn’t tell the whole story because the anatomy is complex.
The navicular bone cannot be considered in isolation. It is an integral part of both the distal interphalangeal (DIP) joint and the podotrochlear apparatus and is closely related to the deep digital flexor tendon (DDFT).
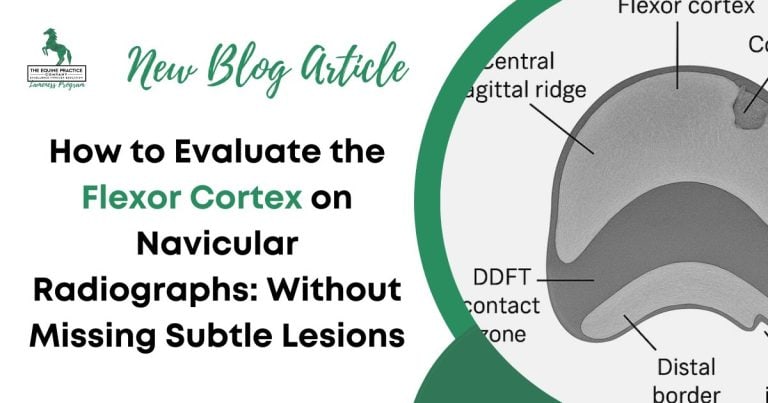
A well-positioned set of navicular radiographs can highlight:
- Synovial invaginations
- Alterations of shape of the navicular bone
- Palmar compact bone irregularity
- Alterations of opacity of the spongiosa
- Entheseophyte formation
- Some distal border fragments
- A bipartite or tripartite navicular bone
- Some fractures
But what they can’t show is just as important:
- Early osseous pathology
- Bone marrow oedema, fibrosis or necrosis
- Injury to related soft tissues such as the DDFT, collateral sesamoidean ligament or distal sesamoidean impar ligament
- Navicular bursa pathology
These limitations aren’t necessarily due to poor technique. They are inherent to the modality. Radiographs are designed to show gross structural change – not early or soft tissue pathology.
A 40% change in bone density is required before radiological changes can be seen. Even with the acquisition of serial radiographs, it is unusual to document changes of navicular bones over time.
In the absence of detectable osseous pathology on radiographs, MRI remains the most appropriate imaging modality, if available and within the client’s budget.
If MRI is not feasible then there is little to be lost by assessing the response to medication of the navicular bursa and/or the DIP joint.
That’s why interpretation must begin with the horse – not the image. If the radiograph doesn’t match what you see on the ground, trust the horse. Use radiographs to support or clarify – not to replace – your clinical judgment.
Signs That Override the Radiograph
When a horse presents with lameness associated with palmar foot pain, and the radiographs are normal —or inconclusive—there are clinical findings that carry more diagnostic weight than any image.
In these moments, your job isn’t to “see more” on the screen. It’s to pay closer attention to the horse.
Here’s what overrides a normal or borderline radiograph:
1. Consistent Lameness Apparently Localised to the Palmar Aspect of the Foot
- Bilateral low-grade forelimb lameness
- Worse on hard ground or tight circles
- May not improve with farriery or rest
If these signs persist, don’t dismiss them because the radiographs look fine. The pathology may be functional or soft tissue–based, and may never be seen on radiographs – or only on MRI.
Moreover, low-field MRI also has limitations. Be aware that not all pain is related to detectable structural abnormalities.
Palmar digital nerve blocks are themselves not specific to palmar foot pain. There is the potential to remove pain from the pastern and fetlock regions.
2. Positive Response to a Navicular Bursa Block
Intrathecal analgesia of the navicular bursa is more specific than palmar digital anaesthesia, assuming the response is seen rapidly, but still does not tell you that navicular bone is the primary source of pain.
Pain could originate from closely related soft tissues and more than one may be involved.
A “normal” radiograph in this case doesn’t clear the navicular bone. It means you need to dig deeper.
3. High-Risk Hoof Conformation
- Long toe, low heel
- Broken-back hoof-pastern axis
- Mediolateral imbalance
Even in the absence of structural changes on radiographs, these conformational abnormalities can place abnormal loads on the podotrochlear apparatus, the DIP joint, and related soft tissues.
These include the DDFT, the ligaments attaching to the ungular cartilages (e.g. the chondrocoronal ligament), and the laminar attachments to the distal phalanx.
4. A History That Doesn’t Add Up: Don’t get confused by
- Intermittent lameness
- Poor performance without overt lameness but an insidious shortening of step length
- Discomfort that returns despite rest and corrective shoeing
These are all signs that may reflect palmar foot pain. The absence of radiographic abnormalities should not stop your clinical reasoning.
Common Mistakes and What They Cost
Most misdiagnoses in navicular cases don’t come from poor radiographs. They come from how we interpret them.
Here are the most common mistakes—and what they can cost the horse, the client, and the veterinarian.
1. Over-Reliance on a Lateromedial View
The lateromedial radiograph is essential – but it must be acquired without obliquity to be of diagnostic value – and that is not always easy in the presence of lateromedial foot imbalance.
The ENTIRE radiograph also needs to be read carefully – asking questions – is the palmar compact bone of normal thickness? Is there proximal or distal extension of the palmar compact bone?
Might there be a fragment distal to the navicular bone. Is there a proximal entheseophyte?
Is the compact bone of uniform opacity? Is there a periarticular osteophyte on the proximodorsal aspect of the navicular bone? Is the spongiosa of normal opacity.
Does the DIP joint look normal? Is there modelling of the palmar processes of the distal phalanx. Is the hoof wall distal phalanx distance normal dorsally?
2. Calling It “Normal” Without Enough Views
Two views (lateromedial and dorsoproximal-palmarodistal oblique) are not enough. Without at least three high-quality projections – including a well-positioned skyline – you haven’t finished the assessment of the navicular bone, the DIP joint and the distal phalanx.
Declaring “no navicular changes” based on an incomplete examination can delay appropriate workup or lead to false reassurance.
3. Treating the Radiograph, Not the Horse
It’s easy to get distracted by findings: one enlarged synovial invagination, some mildfocal increased opacity, a small lateral entheseophyte at the insertion of the collateral sesamoidean ligament.
But if the horse is sound and there are no clinical signs—those changes may be incidental.
Conversely, dismissing a horse with clear clinical signs just because the radiograph is “within normal limits” leads to under diagnosis.
4. Using Imaging to Avoid a Difficult Conversation
When you’re unsure, it’s tempting to lean on the radiograph to reassure the client – or to justify a referral. But this can create false certainty.
A better answer:
“The radiographs don’t show major changes, but they don’t rule out pain. Let’s take the next diagnostic step.”
Or:
‘I cannot detect any abnormality but I would like the opinion of a specialist clinician, just to make sure’
5. Failing to Re-image When Things Don’t Add Up
Radiographs are a moment in time and a historical record of what has happened before. If the clinical picture worsens or stays unresolved after farriery or rest, consider repeat imaging.
However, in the case of the navicular bone it is comparatively unusual to detect progression, whereas abnormalities of the DIP joint may become apparent.
Don’t overlook ultrasonography for evaluation of soft tissues.
Some intervention in the interim is potentially beneficial – can foot balance be improved? Can the fit of the shoe be improved? Consider medication.
Case Snapshots: What the Image Didn’t Tell You
No single radiograph ever tells the whole story. These cases illustrate what can happen when you follow the horse instead of being led by the image – and why clinical judgment always comes first.
Case 1: Radiographs Look Normal. The Horse Is Not.
Horse: 10-year-old Warmblood gelding, dressage
History: Subtle, bilateral forelimb lameness. Worse in circles and on hard surfaces.
Diagnostic blocks: Positive response to navicular bursa analgesia
Radiographs:
- Normal palmar compact bone margins
- No significant increased opacity of the spongiosa
- Symmetrical, well-defined synovial invaginations
Follow-up: MRI revealed dorsal fibrillation of the DDFT in the region of the navicular bone and mild increased signal intensity in the spongiosa of the navicular bone, possibly consistent with bone edema.
Outcome: Treated appropriately and returned to work with hoof care and a controlled rehabilitation program.
The radiographs didn’t show it. The horse did.
Case 2: The Films Look Alarming. The Horse Isn’t Lame.
Horse: 12-year-old show jumper, competing sound
History: No lameness, consistent performance at 1.20m level
Radiographs:
- Generalised increased radiopacity of the spongiosa of the navicular bone. Multiple large synovial invaginations restricted to the distal horizontal border of the navicular bone.
- Mild flattening of the palmar margin of the palmar compact bone, lateral to the sagittal ridge
Clinical examination: Normal gait under all circumstances (in hand, on the lunge and ridden), well trimmed and shod; no pads; conventional open shoes; no response to hoof testers.
Outcome: Passed prepurchase examination with radiographic findings noted but not considered currently clinically relevant, but with a caveat that progression may occur. Follow-up 18 months later: still sound.
The horse was telling the truth. The radiographs weren’t the problem.
Case 3: The Grey Zone
Horse: 9-year-old eventer
History: Mild intermittent left forelimb lameness
Blocks: Improved from grade 2/8 lameness to grade 1/8 after palmar digital nerve blocks; sound after palmar blocks at the level of the base of the proximal sesamoid bones
Farriery history: Mediolateral foot imbalance; trimming and shoeing interval six weeks
Radiographs:
- Six variably sized and shaped synovial invaginations along the distal horizontal border of the navicular bone and an additional radiolucent area at the junction of the horizontal and medial sloping border
- Small rounded mineralised opacity distal to the distal medial aspect of the navicular bone
Approach: Hoof balance addressed. Trimming and shoeing interval reduced to 5 weeks. Lameness resolved within 4 weeks with no further intervention.
A conservative approach based on context prevented overdiagnosis and overtreatment.
Takeaway messages for the Field Vet
Radiographs matter. But they don’t tell the whole story. The navicular bone can NEVER be considered in isolation. The biggest mistakes often happen when we let the image speak louder than the horse.
Here’s what to take with you into your next workup:
- Don’t assume normal radiographs mean a normal foot. Radiographic sensitivity is limited, especially in early-stage disease. Normal radiographs do not rule out pain.
- Always correlate imaging with clinical signs. Start with the premise that there must be a cause of pain, but that does not mean that there will be a radiographic explanation.
- Use the full set of views. For the navicular bone this means removal of the shoe, appropriate preparation of the foot and acquisition of lateromedial, dorsoproximal-palmarodistal oblique and palmaroproximal-palmarodistal oblique views.
- Look at the horse and don’t ignore the obvious. If there is poor foot balance address this as a priority. In a non-lame horse do not overinterpret minor radiological abnormalities. If a horse is lame there must be a reason even if there is no detectable radiological abnormality.
- Be honest about uncertainty. If you’re unsure, say so. Get a second opinion about the radiographs.. Repeat the clinical examination. Refer if needed. Better that than treating the wrong problem—or missing the right one.
Final Thoughts
The navicular bone is not always the source of pain in a horse with palmar foot pain. Navicular radiographs are a tool – not a verdict. They help clarify, not decide.
A confident diagnosis comes not from seeing a single feature, but from knowing when that feature fits the horse in front of you.
If you’ve ever looked at a radiograph of a navicular bone and thought, “It looks normal, but the horse is still lame, what am I missing?…” then this masterclass is for you.
Dr. Sue Dyson will walk you through real examples and highlight common pitfalls in image acquisition and interpretation. Have you ever thought that the synovial invaginations along the distal border of the navicular bone may actually reflect distal interphalangeal joint disease?
Dr. Dyson will show you how to link what you see on the radiographs with what’s actually happening in the horse.
Join us – we promise you’ll leave with more confidence in your diagnostic decisions. Go ahead and click the link and we look forward to seeing you at the masterclass.
The principles outlined here reflect teaching and case-based reasoning used in advanced lameness education, including material taught by Dr Sue Dyson in referral and postgraduate clinical settings.