Increased opacity of the spongiosa of the Navicular Bone and entheseous new bone: What do they mean?
This interpretation framework reflects referral-level radiological assessment used in equine lameness practice and aligns with published standards and clinical teaching in advanced equine diagnostic imaging.
The navicular bone is a sesamoid bone, comprised of compact bone surrounding the trabecular bone or spongiosa. In a normal bone, the trabecular bone and the uniformly radiopaque compact bone are clearly demarcated.
Clinical Decision Summary: Increased Opacity of the Navicular Bone
Increased opacity of the spongiosa of the navicular bone is not a diagnosis in itself.
It may represent:
- Adaptive remodelling in response to altered biomechanical loading
- Early or established primary navicular bone pathology
- Artefact related to positioning, beam angle, or exposure
Interpretation should only be made when:
- Lateromedial and skyline projections are correctly positioned
- The palmar compact bone is clearly demarcated
- Opacity is assessed relative to hoof capsule morphology and limb symmetry
- Findings are correlated with clinical signs and diagnostic analgesia
Generalised increased opacity with loss of trabecular definition is more concerning than focal, symmetric adaptive change – particularly in young horses or those with concurrent palmar compact bone thickening.
Radiographic interpretation must always be contextualised within the podotrochlear apparatus as a whole.
The thickness of the palmar compact bone is influenced by the morphology of the hoof capsule and thus the orientation of the navicular bone and the forces applied to it.
If the hoof capsule is upright the thickness of the palmar compact bone of the navicular bone is thinner than in a hoof with a lower heel angle. The proximal aspect of the palmar compact bone may be slightly thicker than distally.
In well-positioned lateromedial (LM) and palmaroproximal-palmarodistal oblique (PaPr-PaDiO) (skyline) images of the navicular bone of a normal horse there is an obvious fine linear pattern within the spongiosa of the navicular bone and the junction between the palmar compact bone and the trabecular bone is obvious.
However, with slight obliquity of a LM image the palmar compact bone will not be clearly demarcated so that the boundary between the trabecular bone and the compact bone is less obvious.
If the x-ray beam is not tangential to the palmar compact bone in the PaPr-PaDiO image, this will also result in apparent poor demarcation of the palmar compact bone and the spongiosa.
These are artefacts and should not be mistaken for pathological changes.
In some mature sports horses in the skyline projection there may be a thin layer of slightly more opaque trabecular bone immediately dorsal to the palmar compact bone which represents an adaptive change to loading.
This may be most obvious in the region of the sagittal ridge where the biomechanical forces on the bone are in several directions.
In two forms of navicular disease there is a generalised increased opacity of the spongiosa and loss of clear demarcation between the trabecular bone and both the dorsal and the palmar compact bone. This increased opacity reflects increased thickness of the trabeculae at the expense of marrow spaces.
This can be seen in relatively young horses, three and four years of age, and in association with this there is generalised thickening of the palmar compact bone.
This form of navicular disease is generally not associated with the development of erosions of the palmar compact bone or osseous cyst-like lesions within the spongiosa.
In older horses there is increased opacity of the spongiosa together with either resorptive lesions in the palmar compact bone and /or osseous cyst-like lesions within the spongiosa.
Therefore when interpreting radiographs there are important questions to ask:
- Is this a true lateromedial view of the navicular bone ? Can I see the sagittal ridge projected palmar to the rest of the palmar compact bone? Are the dorsal borders of the navicular bone superimposed?
- Is this a well positioned palmaroproximal-palmarodistal oblique image? Is the palmar compact bone seen as a single band of radiopaque bone?
- If the answer to all these questions is yes, then you can make a realistic assessment of the opacity of the trabecular bone and determine whether it is normal or abnormal.
- Is the thickness of the palmar compact bone normal relative to the size of the bone and the morphology of the hoof capsule?
- Are there any other radiological abnormalities suggestive of navicular bone pathology such as an osseous cyst-like lesion in the spongiosa?
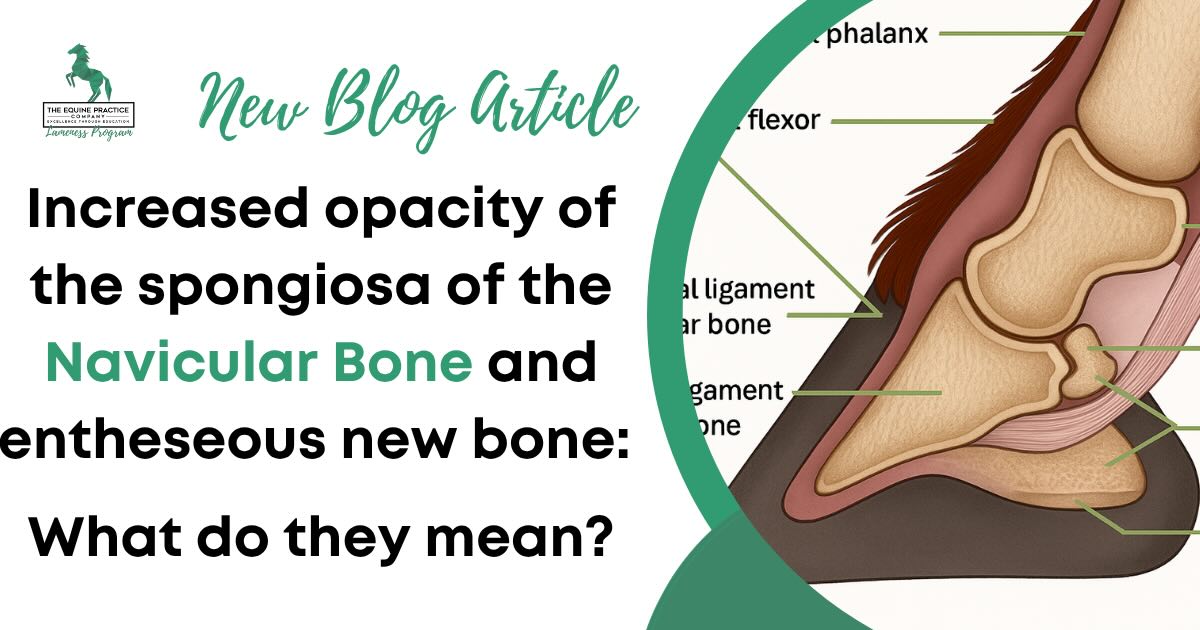
The navicular bone is an integral part of the podotrochlear apparatus. It is attached proximally to the distal aspect of the proximal phalanx (PP) via the collateral sesamoidean ligaments, which cross the proximal interphalangeal joint. Distally, it is connected to the distal phalanx (DP) by the distal sesamoidean impar ligament.
Abnormal stress at ligamentous attachments can result in entheseous new bone formation. This is particularly common at the insertion of the lateral collateral sesamoidean ligament resulting in a smoothly marginated spur of new bone seen on the proximolateral aspect of the navicular bone in a well-positioned dorsoproximal-palmarodistal oblique image. When small this is often an incidental finding of no clinical significance.
However larger spurs, and entheseous new bone proximomedially are more likely to reflect collateral sesamoidean desmitis which may be confirmed using magnetic resonance imaging (MRI).
Some subtle lesions in the palmar compact bone may be associated with increased opacity in the more dorsal spongiosa. Evaluating this region carefully, especially in skyline views, is essential for accurate diagnosis.
Entheseous new bone at the origin of the distal sesamoidean impar ligament is easily overlooked, especially if the fetlock was over flexed during the acquisition of a dorsoproximal- palmarodistal oblique image.
This results in the distal aspect of the navicular bone not being projected over the distal interphalangeal joint space. It is relatively unusual for entheseous new bone at the origin of the distal sesamoidean impar ligament to be an incidental abnormality.
The presence of such entheseous new bone should be verified in a lateromedial image.
Generally, in the absence of other radiological abnormalities of the navicular bone, identification of entheseous new bone can be used to predict likely ligamentous injury, but the presence and severity of injury can only be verified using MRI.

Real-World Cases
Case 1: Increased opacity of the spongiosa as a diagnostic clue
Horse: 4-year-old Warmblood gelding, prospective upper-level dressage horse recently started regular training
History: Moderate bilateral forelimb lameness, worst on a circle on a firm surface
Examination: Lameness abolished by palmar digital nerve blocks; lameness improved by intra-articular anaesthesia of the distal interphalangeal joint within 5 minutes
Radiographs:
- Increased thickness of palmar compact bone in lateromedial and palmaroproximal-palmarodistal oblique images
- Generalised increased opacity of the spongiosa and thickened trabeculae
Follow-up: MRI confirmed diffuse low signal intensity in the spongiosa of the navicular bone in T1 weighted images consistent with abnormal mineralisation.
Outcome: Diagnosed as one type of primary navicular disease
In this case, the radiological abnormalities were a true indication of the primary disease which was confirmed by MRI
Case 2: Incidental Findings
Horse: 11-year-old Quarter Horse, recreational riding
History: No history of lameness, presented for a prepurchase examination
Radiographs:
- A thin layer of increased opacity in the trabecular bone dorsal to the palmar compact bone seen in palmaroproximal-palmarodistal oblique images in both navicular bones
- No palmar compact bone abnormalities
- A small entheseophyte on the proximolateral aspect of each navicular bone
Clinical signs: No lameness or alteration of step length or balance when evaluated in straight lines, on the lunge on soft and firm surfaces and when ridden
Follow-up: Radiographs referred for second opinion
Outcome: No additional abnormalities detected. Horse was recommended for purchase and remained sound at 12-month follow-up
In this case, the localised increased opacity of trabecular bone was adaptive and the entheseous new bone at the insertion of the lateral collateral sesamoidean ligament was considered to be within the normal range. The findings were documented and explained to the purchaser.
These examples reinforce what every experienced equine veterinarian learns with time: radiographic changes are only meaningful when they match the horse. Radiographic findings reflect what has happened to the horse historically.
Radiographic abnormalities of the navicular bone are slow to progress and follow-up radiographs in less than six months are rarely helpful.
Takeaways for the Field Vet
Do not ‘lesion spot’
Read the radiographs in a systematic way, evaluating each margin of each bone and then the internal architecture of the bone.
Describe what you see and then consider whether or not it may be of clinical significance, bearing in mind the morphology of the hoof capsule.
Asymmetry of hoof capsule morphology may be associated with asymmetry of the radiological features of the navicular bone and distal phalanx.
Bear in mind that the navicular bone is part of the podotrochlear apparatus and the associated biomechanical forces.
Appropriate foot preparation is essential to avoid artefacts; this usually require removal of the shoe, paring and cleaning the hoof and the use of packing material to remove potential radiolucent artefacts created by the frog cleft and sulci.
Over packing may result in radiopaque artefacts that mimic lesions.
If you see a radiolucent area apparently within the spongiosa of the navicular bone in a dorsoproximal-palmarodistal oblique image, which is not confirmed in a palmaroproximal-palmarodistal oblique image then repeat the dorsoproximal-palmarodistal oblique image after repacking the foot.
When in doubt send the radiographs for a second opinion. You will learn from this and the outcome will potentially be better for both the horse and the owner, with a correct diagnosis and appropriate management plan.
Be aware that some lesions of the navicular bone cannot be solved, but palmar digital neurectomy may be a valid treatment option in the absence of major deep digital flexor tendon injury, assuming that the lameness is abolished by palmar digital nerve blocks.
Use MRI to confirm when in doubt, assuming that an owner can afford it. There is a subset of horses that have minimal radiographic changes but which do have lesions of the podotrochlear apparatus detectable using MRI.
In some cases, a positive response to a navicular bursa block can be a critical clue – even when radiographs appear normal.
The absence of findings on good quality MR images may be a good prognostic indicator.
Frequently Asked Questions
What does increased opacity of the navicular bone mean?
Increased opacity of the navicular bone reflects thickening of trabeculae within the spongiosa, often at the expense of marrow spaces. This may represent adaptive remodelling or pathological change, depending on distribution, symmetry, and clinical context.
Is navicular sclerosis always pathological?
No. Mild or focal increased opacity may be adaptive, particularly in athletic horses. Generalised sclerosis with loss of trabecular definition is more likely to be clinically significant.
Can increased opacity be an artefact?
Yes. Poor positioning, oblique lateromedial views, or non-tangential skyline projections can create apparent loss of demarcation between compact bone and spongiosa.
Does increased opacity indicate navicular disease?
Not always. It must be interpreted alongside clinical signs, response to diagnostic analgesia, hoof conformation, and other radiographic findings.
When should MRI be considered?
MRI is indicated when radiographic findings are equivocal, lameness persists, or soft tissue injury of the podotrochlear apparatus is suspected.
Final Thoughts
This is exactly the kind of pattern-based reasoning that Dr. Sue Dyson will walk through in her upcoming masterclass. You’ve now covered some of the most commonly misinterpreted features of navicular radiology.
Next, we’ll show you how to bring them together.





